

Abstract
BACKGROUND
Graft-versus-host disease (GvHD) remains an important cause of morbidity and mortality after allogeneic hematopoietic stem cell transplantation, despite the improvements in GvHD prophylaxis. First line treatment of GvHD (acute or chronic) consists of high dose corticosteroids, with a response rate of around 50%. Extracorporeal photopheresis (ECP) is an effective and safe treatment strategy in corticosteroid refractory GvHD, although most of the studies are limited to retrospective series. The main objectives of this study were to analyze the clinical response and impact of ECP therapy in corticosteroid dose reduction.
METHODS
114 patients from 7 Spanish transplantation centers were analyzed retrospectively. The characteristics of the patients are shown on Table 1. A total of 1940 ECP procedures were performed from January-2011 to June-2017 in 65 patients (57%) with acute GvHD (aGvHD) and 49 (43%) with chronic GvHD (cGvHD). Glucksberg and the NIH criteria were used for the diagnosis and grading of acute and chronic GvHD, respectively. All ECP procedures were performed with the off-line system: after the lymphoapheresis, 8-MOP was added to the apheresis product and finally photoinactivated in the Macogenic G1 (Macopharma®) irradiator. During the first 4 weeks, patients underwent 1-2 weekly procedures, followed by 1-2 procedures every 2 weeks and tailored by clinical response. The response was classified as complete response (CR), partial response (PR) or no response (NR). % of the initial corticosteroid dose reduction was registered at the end of treatment.
RESULTS
Patients with aGvHD underwent a median of 13 processes (interquartile range 9-19), and those with cGvHD a median of 19 processes (IQR 13-24). The median number of processes until response was 3 in patients with aGvHD and 4 for patients with cGvHD. ECP was the second line therapy in the 47% of aGvHD cases and 49% in cGvHD. 71% of the cases of aGvHD were grade 3-4, and 69% of the cases of cGvHD corresponded to severe forms.
The overall response rate in aGvHD was 66% (CR 55%), whereas in cGvHD the rate was 67% (CR 22%). The most involved organ was the skin, with a response rate of 80% (CR 68%) in aGvHD and 69% (CR 22%) in cGvHD. In acute digestive GvHD, the response rate was 61% (CR 50%), and 75% (CR 50%) in the chronic form. For liver involvement, response rates were 67% (CR 57%) in acute and 70% (CR 30%) in cGvHD. 80% of the patients with chronic lung involvement showed an overall response (20%CR). At the end of ECP treatment, 71% of the patients treated for aGvHD and 61% of patients with cGvHD were able to reduce the corticosteroid dose, with a median dose reduction of 90% and 100% in all patients, respectively.
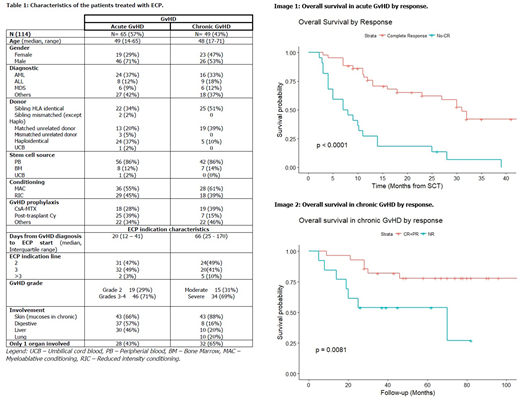
With a median follow-up of 31 months in aGvHD and 68 months in cGvHD, the 2-year overall survival (OS) was 47% and 83%, respectively. Significant OS differences were noted between responding (CR+PR, 2-year OS 62%) and no responding (NR, 2 year OS 18%, HR=2.5, p<0.001) aGvHD patients. Significant differences were also seen in cGvHD between responding (CR+PR, 2 year OS 93%) and no responding (NR, 2 year OS 62%, HR=3.99, p=0.008) patients.
CONCLUSIONS
ECP is a valid therapeutic alternative in patients with corticosteroid refractory acute and cGvHD, with higher CR rates in patients with aGvHD. ECP allowed for significant corticosteroid dose reductions in more than 2/3 of the patients in both GvHD settings, and granted longer OS in responding patients. The results obtained are similar to those published by other groups.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal